


Canada's expanding euthanasia laws: Making the unthinkable thinkable again
Originally published at UK Column


I am republishing this article that I wrote for UK Column last year as tonight I will be on a podcast with Dr. Piers Robinson and Dr. Aaron Good to discuss the current left/right paradigm and how to break through the cognitive dissonance to a healthier understanding of the power behind the breakdown of society across all sectors.
You can listen to the article at the UK Column website.
You can read the article I co-wrote with Piers Robinson - Understanding Power Dynamics and Moving Beyond Divisions: Covid–19 through to Ukraine and Israel/Palestine.
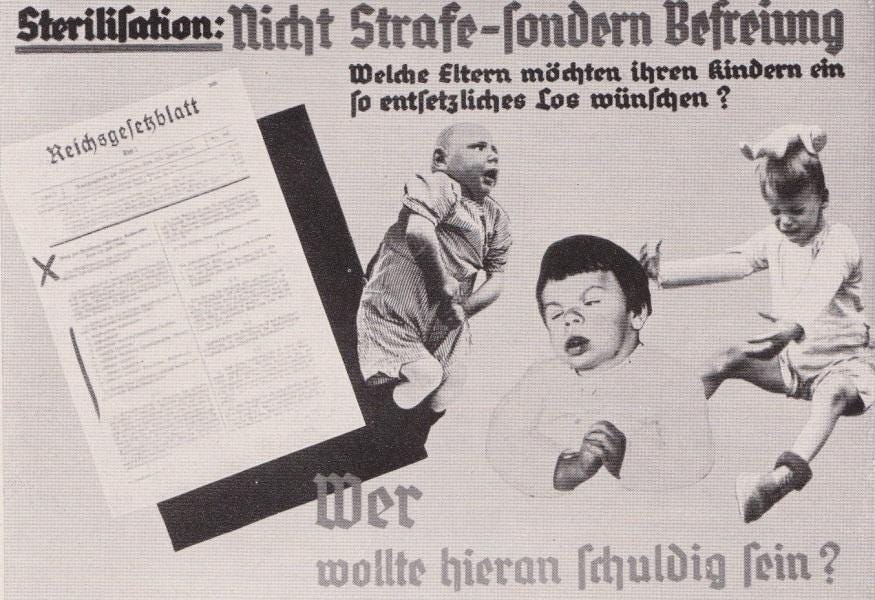
I have added an explanation of the Blue Whale symbolism in the Euthanasia advertising featured in the article. (Image above is taken from that advertisment)
****
“Much that is now unthinkable may at least become thinkable.” Julian Huxley, brother of Brave New World author Aldous Huxley and president of the British Eugenics Society (1959–62), said this when he founded and was Director-General (1946–48) of UNESCO (the United Nations Educational Scientific and Cultural Organisation). The mandate for the new organisation was set out clearly in Huxley’s 1946 UNESCO: Its Purpose and Its Philosophy:
The moral for UNESCO is clear. The task laid upon it of promoting peace and security can never be wholly realised through the means assigned to it—education, science and culture. It must envisage some form of world political unity, whether through a single world government or otherwise, as the only certain means of avoiding war […] in its educational programme it can stress the ultimate need for a world political unity and familiarise all peoples with the implications of the transfer of full sovereignty from separate nations to a world organisation. [Emphasis added]
What Huxley was describing was a stark vision of the post-war future. It is a future that is now upon us with the post-Covid-19 Great Reset that is being formulated by Klaus Schwab and the World Economic Forum oligarchy. Huxley advocated that “genetic stupidity, physical weakness, mental instability and disease proneness” were a “dead weight” for the human species and an obstacle to real progress:
At the moment, it is probable that the indirect effect of civilization is dysgenic instead of eugenic, and in any case it seems likely that the dead weight of genetic stupidity, physical weakness, mental instability and disease proneness, which already exist in the human species will prove too great a burden for real progress to be achieved.
Thus, even though it is quite true that any radical eugenic policy will be for many years politically and psychologically impossible, it will be important for UNESCO to see that the eugenic problem is examined with the greatest care and that the public mind is informed of the issues at stake so that much that is now unthinkable may at least become thinkable.
Canadian historian and author Matt Ehret has pointed out that:
Even though thirty U.S. States and two Canadian provinces had legalised eugenics policies (including forced sterilisation of the unfit) between 1907 [and] 1945, the statistical science and political application of eugenics ground to a screeching halt by the end of World War II and, as Huxley iterated in his manifesto, something new had to be done.
Ehret maps out Huxley’s relationship with the London Tavistock Clinic (1930–50; not to be confused with the still-extant Tavistock Institute of Human Relations, nor with the present-day Tavistock and Portman Foundation NHS Trust, which oversees mental health services in North London and which was recently the subject of a UK Column interview). The Tavistock Clinic of the 1930s and 1940s was led by a psychiatrist, Colonel (later Brigadier-General) John Rawlings Rees—a strategic planner of mental health who has been of interest to Brian Gerrish and other UK Column authors for over a decade. Tavistock as a broad undertaking can be best understood, Ehret writes, as the “psychiatric branch of the British Empire established in 1921 which innovated psychiatric techniques using mixtures of Pavlovian behaviourism and Freudian theories to influence group behaviour in a variety of ways.”
Rees was joined by a Canadian psychiatrist named George Brock Chisholm. In 1948, Chisholm founded a UN-affiliated body called the World Health Organisation (WHO) with the aim of allegedly promoting mental and physical health of the world. As Ehret points out, Chisholm’s mission was effectively the eradication of monotheistic religion, family and patriotism. Eight years after the WHO was founded, Chisholm stated:
To achieve world government, it is necessary to remove from the minds of men their individualism, loyalty to family tradition, national patriotism and religious dogmas.
With the WHO and UNESCO established as partners in the endeavour to make the unthinkable thinkable, a third organisation entered the cartel. The World Federation of Mental Health was also created in 1948, and put in charge of it was none other than Brigadier-General John Rawlings Rees—appointed to the post by Montagu Norman, Director of the Bank of England and co-founder of the Bank for International Settlements, who had created the World Federation as an extension of his own British National Association for Mental Health.
Jim Keith, author of Mind Control, World Control: The Encyclopedia of Mind Control, writes:
The relation of eugenics to British psychiatry bears examination. The primary controlling body for psychiatry in England is the British National Association for Mental Health (NAMH), formed in 1944, and initially run by the mentally unstable Montagu Norman, previously of the Bank of England. The group originally met at Norman's London home, where he and Nazi Economics Minister Hjalmar Schacht had met in the 1930s to arrange financing for Hitler.
The U.S. technical coordinator to the conference that created the WFMH made the new organisation’s origins clearly known. Nina Ridnour wrote that “the World Federation for Mental Health […] had been created upon the recommendation of the United Nations World Health Organization and UNESCO because they needed a non-governmental mental health organisation with which they could cooperate.”
Matt Ehret’s 2021 article How the unthinkable became thinkable: Eric Lander, Julian Huxley and the awakening of sleeping monsters describes the unthinkable alliance thus:
Over the ensuing years, UNESCO, the WHO and WFMH worked in tandem to coordinate hundreds of influential sub organisations, universities, research labs, and covert science including the CIA’s MK Ultra in order to bring about the desired “mentally healthy” society cleansed of its connections to Christianity, faith in truthfulness, national patriotism or family.
This is not merely of historical interest. A recent article in The Conservative Woman aptly describes the Great Reset as the Great Regression:
Eugenics (the devaluing of life into a commodity) is a growing theme in the propaganda of the globalists. You and I are disposable entities, with limited use. If not functioning well enough to provide the labour, service and taxes they want, and becoming a burden on the state, then why not kill us off?
Death reborn: Canadian Medical Assistance in Dying (MAiD)
In 2016, Canada, with Justin Trudeau’s administration in office, passed Bill C–4, legalising medical euthanasia and physician-assisted suicide—together referred to by Canadian public bodies as medical assistance in dying (MAiD). By November 2020, more than 19,000 individuals nearing the end of life had been voluntarily euthanised.
In March 2021, the law was amended by Bill C–7, which permits assisted euthanasia for patients whose death is not reasonably foreseeable. In 2021, it is estimated that more than 10,000 people were assisted in killing themselves in Canada.
The Canadian federal expert panel on the application of MAiD for mental illness has recommended mental illness be grafted onto the MAiD framework without any legislative changes in March 2023. The first report of the federal special joint committee on MAiD suggests it will not only ignore all the problems caused by MAiD, but also further entrench and expand MAiD in Canada.
It was anticipated in an article in the Psychiatric Times when Bill C–7 was new that the legislative change would provide, not prevent, suicide for some mentally ill patients. The article highlighted the threat to ethical norms in psychiatry and reviewed comparable laws in various other countries:
Currently, several countries, such as Belgium, the Netherlands, Luxembourg, and Switzerland, allow patients who are suicidal to receive death by either lethal injection (euthanasia) or a self-administered prescription for lethal medication (assisted suicide). In 2002 Belgium, the Netherlands, and Luxembourg (all three [being] collectively known as Benelux) legalised both these practices. Laws in those countries permitted voluntary death for patients whose physical or psychological suffering was unbearable and could not be effectively treated by means that were acceptable to them. A terminal condition was not a necessary criterion.
According to the article, this led to psychiatric patients having suicide, rather than preventive therapy, provided to them. Between 100 and 200 patients with psychiatric disorders are being euthanised annually in Benelux as a whole.
In concerned response to those developments abroad, the American Psychiatric Association issued a position statement in 2016:
A psychiatrist should not prescribe or administer any intervention to a non-terminally ill person for the purpose of causing death.
The traditional role of a psychiatrist is to prevent patient suicide. The changes to assisted suicide laws, particularly in Canada, threaten to override these ethical standards.
Mental illness is something that many people struggle with, especially in an increasingly oppressive and disenfranchised dystopia that has been rolled out in the form of the Covid–19 response. These Covid consequences include lockdown, mandatory vaccination, harsh economic sanctions against dissidents and increased homelessness, child abuse, depression, drug abuse—and, yes, suicide, associated with the disproportionate measures to curtail a virus promoted as a ‘deadly pandemic’.
The Ottawa régime of WEF Young Global Leader Trudeau—Liberals and Nazi sympathisers aided by the Bloc Québecois—forcibly shut down debate and passed Bill C–7, which included the amendment approving euthanasia for those suffering exclusively from mental health issues—issues in many instances brought on or exacerbated by the Trudeau lockdown package during the Covid two-year madness that began in early 2020.
Carla Qualtrough, Federal Minister of Employment, Workforce Development and Disability Inclusion, has recently expressed her disquiet at the Canadian status quo:
[I]t should not be easier to access a medically assisted death than to get a wheelchair—but it is.
Experts have been predicting a “pandemic” of mental illness and depression as a result of the Covid–19 project, and now that it has materialised, the same governments that introduced the measures designed to send their populations into a psychiatric free-fall are now offering suicide—funded and facilitated by the state and by not much else. In Canada, there is virtually no alternative palliative care available; the fast track is to death. Alex Schadenberg of the Euthanasia Prevention Coalition summed up Bill C–7 as follows:
Bill C–7 removed the requirement in the law that a person’s natural death be reasonably foreseeable in order to qualify for assisted death. Therefore, people who are not terminally ill could die by euthanasia. The Truchon decision only required this amendment to the law, but Bill C–7 goes further.
Bill C–7 permits a doctor or nurse practitioner to lethally inject a person who is incapable of consenting, if that person was previously approved for assisted death. This contravenes the Supreme Court of Canada Carter decision, which stated that only competent people could die by euthanasia.
Bill C–7 waives the ten-day waiting period if a person’s natural death is deemed to be reasonably foreseeable. Thus a person could request death by euthanasia on a “bad day” and die the same day. Studies prove that the “will to live fluctuates”.
Bill C–7 creates a two-track law. A person whose natural death is deemed to be reasonably foreseeable has no waiting period, while a person whose natural death is not deemed to be reasonably foreseeable would have a 90-day waiting period before being killed by lethal injection.
Bill C–7 (originally) falsely claimed to prevent euthanasia for people with mental illness. The euthanasia law permits MAiD for people who are physically or psychologically suffering that is intolerable to the person and that cannot be relieved in a way that the person considers acceptable. However, mental illness, which is not defined in the law, is considered a form of psychological suffering. Now that parliament amended Bill C–7 to specifically permit euthanasia for mental illness, at least the charade has lifted.
Canada leading the way in global depopulation campaign?
Ontario resident Fred Haight points out the confusion over the terminology surrounding assisted death:
Statistics on euthanasia can be confusing, as there are many different forms of it.
"Passive euthanasia" refers mostly to the patient's supposed "right" to refuse "extreme" life-saving measures in the event of a heart attack, or other emergency.
"Physician-assisted suicide" refers to when doctors give prescriptions to patients that will allow them to end their own lives.
"Voluntary Active Euthanasia" refers to when a physician kills the patient, with consent, usually through lethal injection.
"Involuntary Active Euthanasia" is when a doctor makes the decision for the patient.
These all get blurred, as one might expect.
In the neighbouring USA, to the best of Haight’s knowledge, ten states and the District of Columbia have enabled “physician-assisted suicide” where the doctor prescribes the fatal medications. Often, a life expectancy of less than six months is a requirement. Of the other forty states, thirty-six have outlawed it and four have no clear laws on the matter. Active euthanasia is currently outlawed in all fifty states and in D.C. (Statistics are from July 2022.)
Haight describes the procedure as physician-implemented homicide, not physician-assisted death. The actual procedure is as follows:
Step 1: Midazolam 10–20 mg 2–4 ml of 5 mg/ml preparation (pre-anaesthetic, induces sleep in 1–2 minutes).
Step 2: Lidocaine 40 mg 4 ml of 1% preparation; pause to allow effect (reduces possible burning in a peripheral vein due to Propofol).
Step 3: Propofol 1000 mg 100 ml of 10 mg/ml preparation (loss of consciousness within ten seconds, induces coma in 1–2 minutes; death may result from the Propofol but Rocuronium is always given.).
Step 4: Rocuronium 200 mg 20 ml of 10 mg/ml preparation (cardiac arrest after Rocuronium injection usually occurs within five minutes of respiratory arrest).
Abuse of medical ethics and vulnerable patients at risk of choosing death over palliative care
Dr Ramona Coelho is a Canadian family physician whose practice specialises in the care of patients living with mental illness and disability. She was an expert witness before the House and Senate committees examining the bill to extend MAiD, and appeared as an expert before the federal special joint committee on MAiD. She is a founding member of Physicians Together With Vulnerable Canadians.
In July 2022, the London Free Press (Ontario) published an article by Coelho entitled Medical assistance in dying overused in Canada even before expansion. Coelho gives clear examples of MAiD abuse based on evidence provided by doctors, a patient and family members:
“A man was admitted to hospital after suffering a small stroke affecting his balance and swallowing. He was feeling down and isolated due to a COVID-19 outbreak on his ward. The stroke neurologist anticipated he would be able to eat normally and regain most of his balance. Psychiatry diagnosed an adjustment disorder but noted his prognosis was very good. The patient then requested MAiD. Neither of his MAiD assessors had expertise in stroke rehabilitation and recovery. Because he was temporarily eating less, the MAiD assessors decided he could die right away instead of waiting the required 90 days for those living with disabilities despite having no terminal co-morbidities. He received MAiD the following week. This man died alone and depressed and before he had tried proper therapy or reached maximal recovery.”
“A 71-year-old widower was admitted to a Southwestern Ontario hospital after a fall. His family says that during his admission he contracted an infectious diarrheal illness. He was humiliated by staff for the smell of his room, his family said. He developed a new shortness of breath that was not comprehensively assessed. In this context, a hospital team member suggested he would qualify for MAiD. The team said he had end-stage chronic obstructive pulmonary disease and it was terminal. The patient was surprised by the diagnosis but trusted the team. Within 48 hours of his first assessment, he received a medically assisted death. Post-mortem testing showed he did not have end-stage COPD. His family doctor, when notified of his death, also stated he did not have end-stage COPD, but the team had failed to contact her when they were assessing his history.”
The level of coercion involved in these decisions by vulnerable patients in a weakened and perhaps severely humiliated state is terrifying. The decisions were evidently also based on inaccurate information; an abuse of trust by the medical professionals involved. As Coelho points out, “[t]here is no safeguard in the legislation that protects marginalised Canadians (victims of ageism, racism, or ableism) from MAiD being raised as a 'treatment option'”.
Coelho describes the normalisation of MAiD by media outlets: CTV ran a W5 story showcasing a man’s MAiD provision. A patient of Coelho’s let her know that the story was very appealing and that MAiD might be a good option for her. Coelho explained:
This patient is in her midlife and has a recent onset mild spinal cord injury [for] which she hasn’t had time to adjust, receive any peer support or proper symptom control. She would prefer to die than be poor and she is aware the government won’t provide what she needs to live with her new disability.
Unlike other countries that have legalised assisted euthanasia, Canadian doctors are apparently not obliged to focus on alternative medical or social-support options that will relieve patient suffering; they are enabled to offer death as the primary solution.
The case of Amir Farsoud has shocked Canadians into questioning the expansion of assisted dying into the realm of mental health, especially in the current unforgiving economic conditions globally. Farsoud is a disabled 54-year old who was approved for MAiD by his GP (family doctor). He was about to be made homeless and had no financial means to survive in Canada. In November this year, he needed one more doctor’s signature for his killing to be legal in 90 days time. In an interview with Toronto-based City News, he said:
I don’t want to die. But I don’t want to be homeless [i.e., am determined not to be homeless] more than I don’t want to die.
Luckily for Farsoud, strangers stepped in to help him after hearing his tragic story and raised C$60,000 through a GoFundMe campaign to prevent his suicide. What is shocking is that it took the efforts of the media and public campaigning to provide solutions, while the medical professionals and government agencies stood idle.
Other such cases can be found here, here, here, here and here.
Euthanising babies up to a year old
Dr. Louis Roy, from the Quebec College of Physicians, told the Commons' Special Joint Committee on Medical Assistance in Dying (MAiD) in October that his organisation believes MAiD can be appropriate for infants up to age one who are born with “severe deformations” and “very grave and severe medical syndromes whose life expectancy and level of suffering are such that it would make sense to ensure that they do not suffer given that the possibility of survival is nil.”
Dr Roy was actually citing a statement published by the college in December 2021.
After reflecting on expanding eligibility criteria for MAiD, the college announced it supported the idea of newborn euthanasia in cases with a very poor prognosis and “extreme suffering that cannot be relieved.” It also supported extending MAiD to 14- to 17-year-olds and encouraged more public discussion about endorsing euthanasia for seniors “tired of living.”
In the same October address, Dr. Roy reiterated that MAiD may also be expedient for the elderly who are “tired of being alive”. The needless deaths and abuse of the elderly abandoned in care homes was a common feature of the Covid–19 response in most countries that applied such inhumane measures.
The same elderly Canadians must now fear being fast-tracked to suicide if they express a world-weariness that is understandable when governments and health services have been increasingly neglecting their care and support for decades. There is a dark pattern developing of devaluing ruling-class-designated “defective” members of society and finding ways to do away with them under cover of prevention of their suffering.
MAiD is replacing medical treatment and government assistance for those with social, economic and psychiatric issues.
Carla Qualtrough, the above-quoted Canadian Minister for Employment, Workforce Development and Disability Inclusion, is among those hotly contesting the inclusion of infants in the MAiD programme. She finds the suggestion of infant suicide to be “shocking and unacceptable”.
Qualtrough has also referred to the cases of people with disabilities who are registering for MAiD because they are unable to find housing or adequate home care:
Working with the disability community and hearing very regularly that people's options around MAID are being driven by lack of social supports is devastating,
Krista Carr, Executive Vice-President of Inclusion Canada, has said:
An infant cannot consent to their own death. This isn’t MAiD, this is murder.
“Mature minors” also targeted for suicide watch
There is also talk of MAiD being extended to include Canadian “mature minors” aged 14 to 17 years old. Dr Ramona Coelho has asked:
The lack of evidence to support safe practice, and the risk of suicide contagion in teenagers, raises the question: why the rush to make MAiD available for children?
Suicide contagion among teenagers is an issue that has exercised UK Column for more than a decade. Coelho goes on to ask how MAiD can be kept from “being used as a tool to absolve governments of their obligation to provide for those living in poverty, with disability, or with mental illness their equal rights as citizens to health, economic security and life?”
A responsible and humane healthcare network should be looking to decrease suicide not increase it in any society, surely? As Coelho says, “[t[he federal committee on MAiD should slow down, consider the evidence, and not push for expansion to children.”
Coelho asks ,“What are the potential dangers of expanding MAiD to children?” She answers her own question:
One is teenager suicide contagion. There is evidence that messages that promote suicide, and knowing someone who has engaged in self-harm or suicide, both raise the risk of teenage suicide contagion. Indigenous youth are particularly at risk because of an already high suicide rate resulting from longstanding injustice. Indigenous stakeholders have repeatedly demanded support from the federal government for the implementation of suicide prevention and mental wellness strategies in their communities. These demands have not been adequately met and in many cases, ignored, while the federal government instead focuses on making suicide access easier for youth, including Indigenous youth.
The same article by Coelho states:
The Council of Canadian Academies Expert Working Group on MAiD for Mature Minors notes that there is a lack of evidence on how MAiD for children will affect families. It noted there is no robust evidence that captures the voices of youth on this matter including views of minors with disabilities, Indigenous youth, and/or those in the child welfare system. It cites a paucity of international evidence on which to draw conclusions as well.
Below is an excerpt from a report by journalists Clayton and Natali Morris on their Redacted YouTube channel, covering the potential inclusion of ‘mature minors’ in MAiD.
Glorifying suicide: making euthanasia hip for the liberal crowd
La Maison Simons, a Canadian fashion house, has recently produced a promotional video glorifying suicide. The advert presents assisted death as the “most beautiful exit”. The young woman who is about to be helped to kill herself informs you that dying in a hospital is not natural, not soft, in these moments you need ‘softness’. Killing softly, apparently, is a reference to the concoction of drugs that is introduced into the body to kill her, first putting her in a coma before inducing cardiac arrest. How natural is a medically assisted death?
Shortly after Canada’s Thanksgiving Day on 10 October, a 37-year-old woman named Jennyfer was assisted to commit suicide. It was her death that prompted La Maison Simons to launch its macabre advertising campaign to sell fashion and home decor to people who can afford them and who have homes to decorate. Euthanasia thus becomes performance art in a ghoulish PR stunt. The target audience is the upper echelons of society, the wealthy, the privileged.
UPDATE from the Telegram Channel of Robin Monotti + Cory Morningstar:
In the full length promotional video commissioned for Simons, a beautiful, mystical blue whale appears in the frame 5-6 times. This could mean different things to different people. To a child or young adult, the association may be something that many adults are completely unaware of.
The Blue Whale Challenge is a suicide "game" that first appeared on social media platforms... The challenge occurs over the course of 50 days, during which "players" are instructed by "administrators" to engage in daily tasks involving increasingly injurious forms of self-harm. The name of the challenge originates from an unexplained phenomenon wherein whales, highly social animals that travel in herds, stray from the herd and beach themselves in a seemingly deliberate manner, causing their demise...
Social media will evolve and continue to give rise to cultural trends and fads of all kinds; all of these are forms of contagion. But clearly, contagion promoting self-harm and suicidality cannot be tolerated... Best practices should be followed by all media when broaching these issues, including avoiding details about how a specific suicide took place, sharing the content of a suicide note, or providing personal details about the individual who died. Most importantly, self-harm and suicide should never be glamorized or romanticized. Additionally, all discussion of suicide in the media should reinforce that coping skills, support, and treatment are effective tools to thwart this behavior.
The Blue Whale Challenge is an example of how modern constructs like social media can glorify self-harm and suicide, thereby perpetuating an age-old problem like suicide contagion. Young people are particularly vulnerable.
Euthanasia for the homeless, the depressed, the poverty-stricken, the down-and-outs is a terrible choice that they are induced to conclude they have to make because they are given no other apparent option. They are abandoned by their government and their health support system to a death that is only better than the living hell that is their life. A recent article in the Spectator, Why is Canada euthanising the poor?, drew the same conclusion:
Since last year, Canadian law, in all its majesty, has allowed both the rich as well as the poor to kill themselves if they are too poor to continue living with dignity. In fact, the ever-generous Canadian state will even pay for their deaths. What it will not do is spend money to allow them to live instead of killing themselves.
Peter Simons, the former CEO of La Maison Simons, claimed that the advertisement epitomises the company’s values and was made to help build “human connection” and encourage people to be more moral—to “help build the communities we want to live in tomorrow, and leave to our children”. He praises his own courage for promoting this message.
Perhaps the company should have established homeless shelters or offered more jobs for the disabled or mentally handicapped, or funded health clinics for the many who have no access to medical support? Perhaps this would have improved society’s morals far more than encouraging and normalising suicide for those who are without hope or a future?
For Jennyfer, it was clearly a choice—but if this video increases the normalisation of suicide as an answer to the misery that people are increasingly being forced to endure, then it has done a great disservice to the most vulnerable in our societies.
Peter Simon's statement is chilling in that it claims his company is shaping the society we leave to our children and that we want to live in tomorrow. If our lives are to be shaped by consumerism and a capitalist death culture that marginalises the poor and needy, no thank you.
The dehumanisation of victims and the death salesmen
In 1941, Hitler’s propaganda chief, Josef Goebbels, commissioned a film to normalise the criminal Nazi T4 euthanasia programme. The film, Ich klage an (I Accuse), was a huge commercial success watched by more than 18 million people. It is the heartbreaking story of a beautiful young woman with multiple sclerosis who begs her husband, a doctor, to kill her. The husband carries out her wishes and is later put on trial.
This romanticised scene-setting was far removed from the gruesome reality of the Nazi euthanasia programme, which exterminated between 275,000 and 300,000 mentally or physically disabled victims from 1939 to 1945.
During the Nuremberg medical trials, Hitler’s personal physician, Dr Karl Brandt, defended the euthanasia programme with the following words in 1948, and they were to be his last:
I think that everybody who has any imagination will turn away shudderingly (sic) from the mis development of nature. These people live under cruel imagination and persecution manias, partly without any consciousness, and one can safely say that every one of these people if they for one clear moment would be able to see their real condition would be very grateful to be dead [...]
I do not feel that I am incriminated. I am convinced that I can bear the responsibility for what I did in this connection before my conscience. I was motivated by absolutely humane feelings. I never had any other intention. I never had any other belief than those poor miserable creatures—that the painful lives of these creatures were to be shortened. [Emphasis added]
The Nazis wanted to rid Germany of the “resource-draining” members of the population. Is what we are seeing develop in Canada with the proposed expansion of MAiD any different?
In 2020, an unnamed Canadian senator commissioned a report on the potential financial impact of expanding MAiD in terms of a cost-benefit analysis. The resultant government document—Cost Estimate for Bill C–7 Medical Assistance in Dying—claimed that existing MAiD legislation was probably saving C$87 million in taxpayer-funded healthcare costs. ‘Broadening eligibility for medical assistance in dying’ would potentially provide further savings of an estimated C$62 million—the monetisation of death.
Justin Trudeau, Chrystia Freeland and their Nazi connections
On 25 November, Russian Foreign Ministry spokesperson Maria Zakharova published a brief opinion piece, of which the following is an excerpt:
Canada legalised physician-assisted suicides in 2016. The number of people who wish to be euthanised has been growing annually. In all probability, Canada will reach 50,000 such deaths a year—an achievement worthy of a country that took care of and gave refuge to the surviving Nazi scum.
I would remind you that the Third Reich with its Aktion T4 programme (Tiergartenstraße-4) was the first state to introduce euthanasia on a mass scale. Apart from racial prejudice, the Nazis proceeded from economic considerations. It was expensive to pay for people requiring treatment. This was a tax burden.
According to a document found in the Hartheim Euthanasia Centre in Nazi Germany, 70,273 people were killed under the Tiergartenstraße-4 programme by September 1, 1941. An unknown Nazi clerk noted with chilling pragmatism: “Considering that these patients could live for another ten years, this is a saving of 885,439,800 Reichsmarks in total.”
Is the motivation of neoliberal Ottawa different from that of the Reich? Judge for yourselves.
I met with Maria Zakharova in Moscow in November 2016. During the meeting, she became visibly emotional as she described the suffering of her grandparents during the “Great Patriotic War” at the hands of the Nazis. For the majority of Russians, the re-emergence of Nazism in Ukraine on Russian borders, protected, armed, trained and promoted by the West—and with Canada playing an instrumental role—is an intolerable aberration.
Justin Trudeau has close WEF ties to Klaus Schwab, who himself has Nazi origins, and Chrystia Freeland, Deputy Prime Minister, also has much-denied ties to the German Nazi Party and the modern day ultra-nationalist Banderites in Ukraine: her maternal grandfather was a Nazi collaborator and promoter of Nazi doctrine through Ukrainian Nazi-sympathetic media channels.
This grandfather, Michael Chomiak (a later Anglo-Polish spelling of his name, which was originally spelt the Ukrainian way as Mykhailo Khomiak) was editor-in-chief of the Kraków News (Ukrainian: Krakivs’ki Visti), which was known to be vehemently anti-Semitic and published Nazi propaganda on a daily basis, was kept afloat with German financial aid and was pushed to the forefront of media exposure by Joseph Goebbels himself.
Journalist and historian John Helmer has written extensively on the subject and he has reported on German military records found in a Polish government archive in Warsaw:
revealing that Michael Chomiak [...] volunteered to serve in the German invasion of Poland long before the German Army attacked the Soviet Union and invaded Ukraine. Chomiak’s records show that he was trained in Vienna for German espionage and propaganda operations, then promoted to run the German press machine for the Galician region of Ukraine and Poland during the four-year occupation. So high-ranking and active in the Nazi cause was Chomiak that the Polish intelligence services were actively hunting for Chomiak until the 1980s—without knowing he had fled for safety to an Alberta farm in Canada.
Richard Sanders, editor of Press for Conversion and member of the Coalition to Oppose the Arms Trade, went further in his investigation into Canada’s role in keeping Nazism alive after 1945. Sanders concluded that the personal Freeland Nazi connections were a diversion from the more sinister reality that Canada had imported tens of thousands of “displaced persons” of Ukrainian heritage in the years following the Second World War. In 2017, he wrote:
Many thousands of these immigrants harboured such extremely nationalistic ideologies towards Ukraine that they had sympathised and collaborated with the Nazi regime during the war. Many were pleased to do this because they had been led to believe—by their mass media, the [Uniate] church and other powerful civic institutions—that the Third Reich was a benevolent, liberating force which was assisting them in the noble cause of promoting Ukrainian culture. They also felt a strong affinity to the Nazis because they shared a common worldview which despised two mortal enemies: Jews and communists. This worldview—regarding a Judeo-Bolshevik enemy—was also shared by many mainstream Canadians at that time, including many among this country's top political and religious leaders.
Sanders describes the new Ukrainian Canadians as several thousand veterans from two Nazi-influenced military formations: the Waffen-SS Galicia Division and the Ukrainian Insurgent Army (UPA). This was the military wing of the Organisation of Ukrainian Nationalists (OUN-B) led by the notorious ethnic cleansing Stepan Bandera, who is now iconised in Zelensky’s Ukraine. The ultra-nationalist ideologies that these refugees carried with them still permeate Canada’s political and institutional class. A friend of Freeland's is Paul Grod, the president of the Ukrainian Canadian Congress (UCC). According to Sanders, the UCC “had core national member organisations that represent the leadership of both factions within the OUN, including the more extreme Banderites”.
The Trudeau régime's totalitarian roots came to the surface during the crackdown on dissent during the two-year marathon of the state's Covid–19 response. The Freedom Convoy organisers were brutalised by state security forces, discredited as “right-wing extremists” and had their bank accounts frozen for daring to question Covid–19 measures, including mandatory experimental and high-risk vaccines, that were intended to further victimise the working class and disenfranchised members of Canadian society. Debanking is a term that accurately describes the government collusion with the banking system to target individuals with “adverse” political views in order to intimidate and silence opposition. Does this sound familiar?
Dr. Mark Trozzi, a vehement opponent of the Covid–19 measures, wrote in February 2022:
In addition to invoking the Emergencies Act to use force against the peaceful truckers and citizens protests; the Trudeau regime now also has the Emergency Economic Measures Order. This gross violation of the God-given right to private property, involves freezing the accounts and insurance policies of anyone involved in expressing an opinion contrary to the Trudeau regime's dictates and lies.
Certainly when put in this context, the expansion of MAiD must be rigorously questioned and alarms must be raised.
The unthinkable is back in vogue
Fred Haight summarises the situation thus:
[T]hese and other arguments marshalled in favour of euthanasia in Canada bear a striking resemblance to those made in the past to justify eugenics. At the turn of the 20th century, the fiercest proponents of euthanasia and eugenics were physicians and academics. In the US, Dr Ella K. Dearborn cheerfully called for ‘euthanasia for the incurably ill, insane, criminals and degenerates’. Dearborn thought it entirely reasonable that everyone should pass an examination allowing them to continue living. In 1906, one sociologist noted in the Minneapolis Journal: ‘I would personally rather administer chloroform to the poor, starving children of New York, Philadelphia, Chicago and other American cities, than to see them living as they must in squalor and misery.’
Zakharova put it rather more succinctly when she said:
The abhorrent Nazi interpretation of eugenics was reincarnated in neoliberalism and received an official seal of approval in Canadian law. This is what all progressives are appealing for today.
It should be borne in mind that Bill C–7 permits a doctor or nurse practitioner to lethally inject a person who is incapable of consenting, if that person was previously approved for assisted death. As Zakharova has pointed out:
I’d like to recall a sentence from the Hippocratic Oath: “Neither will I administer a poison to anybody when asked to do so, nor will I suggest such a course.”
Russian philosopher Sergey Shevchenko wrote an article in 2019 entitled Why can’t euthanasia be allowed in Russia?. Shevchenko argues that the reason why is that if medically-assisted death were to be legalised, situations would arise where those unable to afford medical treatment or who are afraid of being a burden to their relatives might be unfairly persuaded to take the assisted suicide route. He writes:
In other words, euthanasia can become an “easy solution” not only for the suffering person but also for both social groups and institutions that are ready to sacrifice a lot in the fight for some economic expediency.
In Canada, Justice Minister David Lametti is being pressured to delay the expansion of MAiD amid growing public and medical professional unease, but he declined to promise any moratorium.
Claiming that substantial resources have been put into the MAiD project (but not into providing alternative health and psychiatric support), Lametti told MPs:
We’ll work in good faith to make sure that Canadians are ready for mental disorder as a sole criterion for seeking MAiD.
In 1940, Canadian poet Earle Birney wrote a poem called David that extolled the virtues of euthanasia. This poem was required reading in high schools across Canada for decades. Canada has danced with orchestrated death for a very long time, and now this subliminal advocacy for legitimising murder as “assisted suicide” has come to the fore again in a very sinister manner.
Canada leads; will the world follow blindly into an inhumane dystopia where the most neglected and abused among us will be exterminated as the world is distracted by perpetual wars, famine and plagues? Will history repeat itself, or will we wake up in time to prevent such horrors haunting the world that our children will be forced to inhabit?
****
Please do consider subscribing to my Substack. I am entirely dependent on public donations and not funded by any organisation or government/government agency. Your support is invaluable and massively appreciated. Thank you x
Coming to the UK in a Canadian way as soon as they can get it pushed through, no two ways about it.
This is also why I hate it when even normally sensible presenters jump on words that our mischief makers of the government have deliberately brought into everyday use. In this case use of "boomers" or even "Gen z". Boomers deliberately put out there to cause a split between older and younger generations and sadly it's worked on a lot. All you read in various comments is if it wasn't for boomers there wouldn't be a pension shortage and the like.
Load of rubbish, if the government hadn't dipped into the future pensioners funds everything would be fine. One way or another whatever department behind this has managed to stir up enough resentment so when they bring in assisted dying, like was spoken about in I think 2020 or could have been 2021, people could have demise parties, get to a certain age ( they thought 65) and you hold a party to say goodbye to family and friends and take your medication to shuffle yourself off this mortal coil with everyone around!!
Some were even suggesting at the age of sixty. This was seriously discussed in the UK while a lot of people were too wrapped up in covid to take a lot of notice.
I always say if a certain word becomes quickly popular in relation to labelling of people, there's an agenda fast coming behind it.
When the massive autistic population comes of age and their free caretakers die of old age, this euthanasia thing is going to seem a logical solution.